P-148: On-demand plerixafor added to high-dose cyclophosphamide and Pegfilgrastim in the mobilization of patients with multiple myeloma: High effectiveness and affordable cost
Professor First Affiliated Hospital of Sun Yat-sen University, United States
Introduction: Upfront single or tandem autologous stem cell transplantation(ASCT) still represents an integral part of treatment for patients with multiple myeloma. It is important to collect enough stem cells for two transplants in the first mobilization.The combination of high-dose cyclophosphamide(CTX) (3g/m2) plus Filgrastim(FIL) and on-demand plerixafor has been considered the effective method as mobilization regimen, but FIL requires daily, multi-injection administration.We adopted a mobilization regimen with CTX combination pegfilgrastim (PEG) and on-demand plerixafor, allowing for a single injection given the long half-life and slow elimination of PEG. Here, we performed a real-world analysis to evaluate the efficacy and cost of high-dose CTX combination PEG and on-demand plerixafor for mobilization in MM patients.
Methods: We retrospectively compared 340 patients whith MM mobilized between August 2008 and December 2022 using the following mobilization strategies:CTX+PEG+/-Plerixafor(n=60), CTX+ PEG ( n=91), CTX+ FIL( n=169), FIL+Plerixafor(n=20). Then the stem cell mobilization and collection results of the four groups were compared
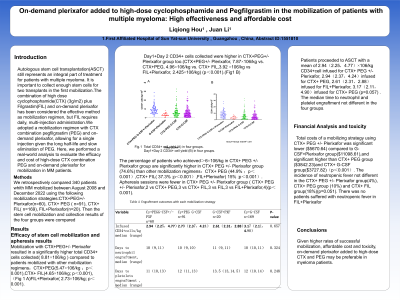
Results: Mobilization with CTX+PEG+/- Plerixafor resulted in a significantly higher total CD34+ cells collected( 8.81×106/kg ) compared to patients mobilized with other mobilization regimens:CTX+PEG(5.47×106/kg ;p<0.001),CTX+ FIL(4.65×106/kg; p<0.001), FIL+Plerixafor( 2.73×106/kg; p<0.001). Day1+Day 2 CD34+ cells collected were higher in CTX+PEG+/- Plerixafor group too.(CTX+PEG+/- Plerixafor, 7.87×106/kg vs. CTX+PEG, 4.96×106/kg vs. CTX+ FIL,3.92 ×106/kg vs FIL+Plerixafor, 2.425×106/kg) (p<0.001).The percentage of patients who achieved>6×106/kg in CTX+ PEG +/- Plerixafor group are significantly higher in CTX+ PEG +/- Plerixafor group (74.6%) than other mobilization regimens:CTX+ PEG (44.9% ;p<0.001),CTX+ FIL( 37.3% ;p<0.001),FIL+Plerixafor( 15% ;p<0.001). Apheresis sessions were fewer in CTX+ PEG +/- Plerixafor group ( CTX+ PEG +/- Plerixafor,2 vs CTX+ PEG,3 vs CTX+ FIL,3 vs FIL+Plerixafor,4)(p<0.001). Patients proceeded to ASCT with a mean of 2.94(2.25,4.77)×106/kg CD34+cell infused for CTX+ PEG +/- Plerixafor, 2.94(2.37,4.24)infused for CTX+ PEG, 2.61(2.31,2.88)infused for FIL+Plerixafor, 3.17(2.11,4.90)infused for CTX+ PEG (p=0.057) . The median time to neutrophil and platelet engraftment not different in the four groups. Total costs of a mobilizing strategy using CTX+ PEG +/- Plerixafor was significant lower ($5670.64) compared to G-CSF+Plerixafor group($11098.61),and significant higher than CTX+ PEG group ($3842.23)and CTX+ G-CSF group($3727.82)(p<0.001). The incidence of neutropenic fever not different in the CTX+ PEG +/- Plerixafor group(4%), CTX+ PEG group (10%) and CTX+ FIL group(18%)(p=0.051). There was no patients suffered with neutropenic fever in FIL+Plerixafor
Conclusions: Given higher rates of successful mobilization, affordable cost and toxicity, on-demand plerixafor added to high-dose CTX and PEG may be preferable in myeloma patients.