Associated Professor Asan Medical Center, Ulsan University College of Medicine Seoul, Republic of Korea
Introduction: We report a patient with CD20-positive light chain-type small cell variant plasma cell myeloma who was misdiagnosed with lymphoplasmacytic lymphoma and did not respond to anti-CD20 immunotherapy.
Methods: Not applicable
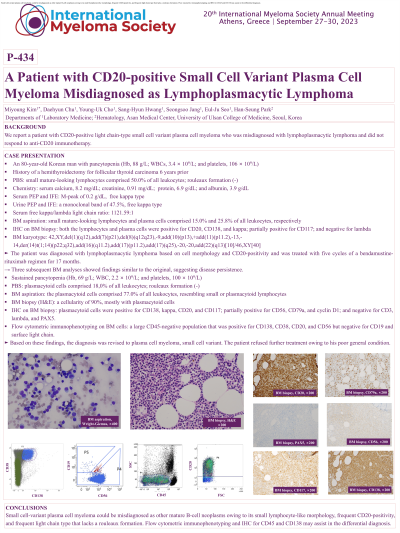
Results: An 80-year-old Korean man with pancytopenia visited our institution in August 2020. He had undergone a hemithyroidectomy for follicular thyroid carcinoma 6 years prior. His complete blood count showed hemoglobin (Hb), 88 g/L; white blood cells (WBCs), 3.4 × 10^9/L; and platelets, 106 × 10^9/L. Small mature-looking lymphocytes comprised 50,0% of all leukocytes; rouleaux formation was absent. In the bone marrow (BM) aspirate, 15.0% of total nucleated cells were mature lymphocytes, and 25.8% were plasma cells. On immunohistochemistry (IHC) of the BM biopsy sample, both the lymphocytes and plasma cells were positive for CD20, CD138, and kappa; partially positive for CD117; and negative for lambda. His serum calcium, creatinine, protein, and albumin levels were 8.2 mg/dL, 0.91 mg/dL, 6.9 g/dL, and 3.9 g/dL, respectively. Serum protein electrophoresis (PEP) and immunofixation electrophoresis (IFE) showed an M-peak of 0.2 g/dL (free kappa type). Urine PEP and IFE showed a monoclonal band of 47.5% (free kappa type). The serum free kappa/lambda light chain ratio was 1121.59:1. The karyotype was 42,XY,del(1)(q12),add(7)(p21),del(8)(q12q23),-9,add(10)(p13),+add(11)(p11.2),-13,-14,der(14)t(1;14)(p22;q32),add(16)(q11.2),add(17)(p11.2),add(17)(q25),-20,-20,add(22)(q13)[10]/46,XY[40]. The patient was diagnosed with lymphoplasmacytic lymphoma based on cell morphology and CD20-positivity and was treated with five cycles of a bendamustine-rituximab regimen for 17 months. Three subsequent BM analyses showed findings similar to the original, suggesting disease persistence. His pancytopenia was sustained with Hb, 69 g/L; WBC, 2.2 × 10^9/L; and platelets, 100 × 10^9/L. Plasmacytoid cells comprised 18,0% of all leukocytes with no rouleaux formation observed; they also comprised 77.0% of the BM aspirate, resembling small or plasmacytoid lymphocytes. The BM cellularity was 90%, mostly with plasmacytoid cells that were positive for CD138, kappa, CD20, and CD117; partially positive for CD56, CD79a, and cyclin D1; and negative for CD3, lambda, and PAX5. Flow cytometric immunophenotyping showed a large CD45-negative population that was positive for CD138, CD38, CD20, and CD56 but negative for CD19 and surface light chain. Based on these findings, the diagnosis was revised to plasma cell myeloma, small cell variant. The patient refused further treatment owing to his poor general condition.
Conclusions: Small cell-variant plasma cell myeloma could be misdiagnosed as other mature B-cell neoplasms owing to its small lymphocyte-like morphology, frequent CD20-positivity, and frequent light chain type that lacks a rouleaux formation. Flow cytometric immunophenotyping and IHC for CD45 and CD138 may assist in the differential diagnosis.

 photo")