P-297: Selinexor, bortezomib, and dexamethasone in patients with previously treated multiple myeloma: updated results of BOSTON trial by prior therapies
Professor University Hospital of Salamanca/IBSAL/CIC/CIBERONC, Salamanca, Spain Salamanca, Spain
Introduction: Increasing use of daratumumab + lenalidomide + dexamethasone (DRd) in the frontline setting for multiple myeloma (MM) has led to more patients (pts) with proteasome inhibitor (PI)-naïve early relapse. ESMO Guidelines endorse a PI-based combination including selinexor, bortezomib, and dexamethasone (SVd) in MM pts with PI-naïve early relapse. Selinexor is a first-in-class, oral XPO1 inhibitor with a unique mechanism of action. SVd is indicated for relapsed and refractory MM (RRMM) in adults who have received at least one prior therapy. We analyzed longer follow-up data from the phase 3 BOSTON trial (NCT03110562) to determine the impact of prior therapies, including PI, on SVd efficacy and safety.
Methods: Eligible pts with RRMM and 1-3 prior therapies were randomized to selinexor QW (100 mg), bortezomib QW (1.3 mg/m2) and dexamethasone BIW (20 mg) (Vd) or standard BIW Vd. A stratified efficacy analysis and safety analysis were performed in subgroups by prior PI therapy and number of prior regimens. Efficacy analyses were based on Feb 2021 data cut and safety analyses on Jun 2022 data cut.
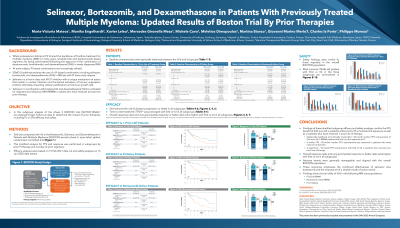
Results: Of 402 pts, 198 received 1 prior line of treatment (LOT) (SVd=99; Vd=99; median ages 67 and 69 y, respectively); 95 were PI-naïve (SVd=47; Vd=48; median ages 68 and 67.5 y, respectively); 123 were bortezomib naïve (SVd=61; Vd=62; median ages 68 y both arms). In pts with 1 prior LOT, mPFS was 21.0 vs 10.7 months for SVD vs Vd (HR 0.62; 95% CI 0.41-0.95, p=0.028). In PI naïve pts mPFS was 29.5 vs 9.7 months for SVd vs Vd (HR 0.29; 95% CI 0.14-0.63, p< 0.001). In bortezomib naïve pts mPFS was 29.5 vs 9.7 months for SVd vs Vd (HR 0.35; 95% CI 0.18-0.68, p=0.002). Overall response rates (ORR) were higher with SVd vs Vd in all subgroups: 1 prior LOT 80.8% vs 66.7%; PI-naïve 76.6% vs 70.8%; bortezomib-naïve ORR 75.4% vs 69.4%. Most common (≥25%) treatment-emergent adverse events (AEs) with SVd vs Vd in pts with 1 prior LOT were thrombocytopenia (61.6% vs 28.6%), nausea (52.5% vs 11.2%), fatigue (45.4% vs 17.3%), peripheral neuropathy (38.4% vs 52.0%), diarrhea (34.3% vs 24.5%), and anemia (30.3% vs 26.5%). Safety findings were similar in the PI naïve and bortezomib naïve subgroups.
Conclusions: Stratified subgroup data from longer follow-up in the BOSTON trial confirm the PFS benefit of SVd over Vd in pts without prior PI or bortezomib exposure as well as pts who have received 1 prior LOT. There was a statistically significant and clinically meaningful ~20 mo median PFS improvement of SVd over Vd in RRMM pts that had no prior exposure to PI and bortezomib, as well as a significant ~10 mo PFS improvement in pts with 1 prior LOT. These outcomes coupled with generally manageable AE profile emphasize the synergy between selinexor and bortezomib and the importance of a double mode of action switch, further supporting SVd use in 1) PI-naïve RRMM pts, 2) bortezomib-naïve RRMM pts, and 3) pts at first relapse.