Assistan Professor Weill Cornell Medicine New York, New York, United States
Introduction: Less than 5% of all multiple myeloma (MM) are diagnosed < 45 years. Previous studies have described the clinical characteristics and validated MM prognostic variables, but the molecular characteristics of this group are unclear.
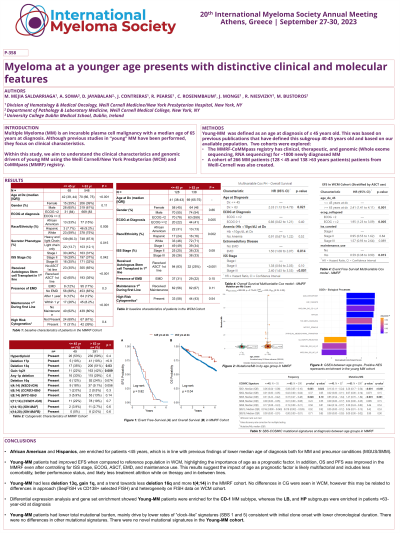
Methods: 129 patients with MM diagnosed at age ≤45 at a single center (Weill Cornell, WCM) were reviewed and compared to a randomly selected group of 101 patients ≥ 63 years. All patients met IMWG MM diagnosis and response criteria. Patients ≤ 45 years (55 patients) in the MM Research Foundation (MMRF) CoMMpass were compared to those ≥63 years (548 patients). The control group age >63 was selected to identify those above the median age and diminish overlap between groups.
Results: African American (AA) were enriched in the ≤ 45 year groups in both cohorts (WCM 31% vs 13%, MMRF 33% vs 15%, p < 0.01). Lower ECOG, higher autologous stem cell transplant (ASCT), and lower ISS were seen in the young subgroup in both cohorts. Age ≥ 63 year at diagnosis was associated with worse PFS in the univariable and multivariable analysis (WCM: HR 3.4, 95CI (1.9 - 6.2) p< 0.01, MMRF: HR 1.6, 95CI 1.05 – 2.3, p 0.03), while worse OS was seen in both cohorts in univariable but only in the multivariable analysis in the MMRF cohort (HR 1.94 (1.05 – 3.6, p 0.03). ASCT, ISS, extramedullary disease, and high-risk cytogenetics were associated with worse PFS/OS. A sensitivity analysis using >45 years at diagnosis (183 patients) as a control in the WCM cohort showed similar results. Lower incidence of deletion 13q and gain 1q in the ≤ 45 years cohort (35% vs 50% p = 0.03, and 22% vs 42% p < 0.01) when compared to the ≥ 63 year cohort was seen. There were no differences in the rate of recurrent translocation, deletion, or mutations in MM. Enrichment of the CD-1 (associated with Cyclin D1) subgroup in the ≤ 45 years subgroup, while the LB (low bone) and HP (associated with hyperdiploidy) were enriched in the older group. Mutational signature analysis was done including all single nucleotide variants, the ≥ 63 year had higher mutational burden (3.8 vs 3.3 mut/Mb, p < 0.01), due to higher count and frequency of clock-like signatures (COSMIC 1 and 5), while there were no differences in other signatures.
Conclusions: Young MM represents a distinct clinical enriched for AA, lower ISS stage and likely higher functional class and physiologic reserve (higher ASCT and lower ECOG), leading to improved PFS/OS, likely derived from better tolerance to highly active therapies and less attrition after progression. We identified a distinct molecular subgroup enriched for CD-1 signature and lower rates of deletion 13q and gain 1q, with a higher mutational burden due to higher clock-like signatures which suggest a later time of disease onset. There were no differences in the rate of recurrent translocation, hyperdiploidy or mutations. Genomic studies focused in AAs/Hispanics germline and somatic factors associated with MM are required to identify the biological origin for the observed differences.